1) What is an anal fistula?
Anal fistula, or fistula-in-ano, is an abnormal connection between the epithelialised surface of the anal canal and the perianal skin and is lined by granulation tissue. There may be single or multiple tracts.
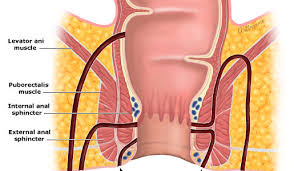
Anal fistulae originate from the infected anal glands, which are located between the two layers of the anal sphincters and which drain into the anal canal. If the outlet of these glands becomes blocked, an abscess can form which can eventually point to the skin surface. The tract formed by this process is the fistula.
2) What causes a fistula?
After an abscess has been drained, a tunnel may persist connecting the anal gland from which the abscess arose to the skin
Symptoms
Pain
Discharge - either bloody or purulent
Pruritus ani - itching
Systemic symptoms if abscess becomes infected
Treatment
There is no definitive medical treatment. Different surgical approaches are available.
There are several options:
LASER FOR FISTULA :This has become most popular and successful treatment of fistula the result of using laser 1470 has increased the comfertablity and healing rate in fistulas
Lay-open of fistula-in-ano(fistulotomy) - this option involves an operation to cut the fistula open.
Fistulectomy- the tract is cored out completely with closure of internal opening
Cutting seton/ksharsutra - If the fistula is in a high position and it passes through a significant portion of the sphincter muscle, a cutting seton may be used.
Fibrin glue injection is a method explored in recent years, with variable success. It involves injecting the fistula with biodegradable glue which should, in theory, close the fistula from the inside out, and let it heal naturally.
Fistula plug involves plugging the fistula with a device made from bovine small intestinal submucosa.
Endorectal advancement flap is a procedure in which the internal opening of the fistula is identified and a flap of mucosal tissue is cut around the opening. and surrounding mucosa is raised to cover the opening Success rates are variable and high recurrence rates.
LIFT Technique - Fistulous tract is identified in intersphincteric plane cut and closed
VAAFT Technique: This technique involves use of an endoscope .
SLOFT :- Sub mucosal ligation of fistulas tract .Fistulous tract is closed in sub mucosal plane
FiLaC :- Fistula laser closure by diode laser
PERFACT ;-Proximal superficial cauterization emptying regularly fistula tract and curettage of tract
Any one procedure does not suit to all fistulas We do all the above procedures depending on type of fistula.